How Left Ventricular Dysfunction Leads to Mitral Regurgitation - Causes, Diagnosis & Treatment
 Oct, 19 2025
Oct, 19 2025
Mitral Regurgitation Severity Calculator
How it works
This calculator uses echocardiographic parameters to determine mitral regurgitation severity based on established guidelines. Enter your EROA (effective regurgitant orifice area) and regurgitant volume measurements to get the severity classification.
Severity thresholds: Mild (<0.20 cm²), Moderate (0.21-0.40 cm²), Severe (>0.40 cm²)
Enter your echocardiographic measurements above to see your MR severity classification
When the heart’s main pumping chamber struggles, Left Ventricular Dysfunction is a condition in which the left ventricle cannot contract (systolic) or relax (diastolic) effectively, lowering cardiac output. This impairment often creates the perfect storm for Mitral Regurgitation, a backward leak of blood from the left ventricle into the left atrium. Understanding why these two problems appear together helps clinicians spot early warning signs, order the right tests, and choose the most effective therapy.
Key Takeaways
- Left ventricular dysfunction (LVD) changes the geometry of the heart, pulling the mitral valve leaflets apart and causing functional mitral regurgitation (FMR).
- Systolic and diastolic LVD have different impacts on the mitral apparatus; systolic failure stretches the annulus, while diastolic stiffening raises left‑atrial pressure.
- Echocardiography, especially 3D and strain imaging, is the frontline tool for quantifying both LVD severity and MR grade.
- Medical therapy (ACE inhibitors, beta‑blockers) can improve ventricular remodeling, often reducing MR severity before surgery is considered.
- When MR remains severe despite optimal medical care, percutaneous edge‑to‑edge repair (MitraClip) or surgical valve replacement becomes necessary.
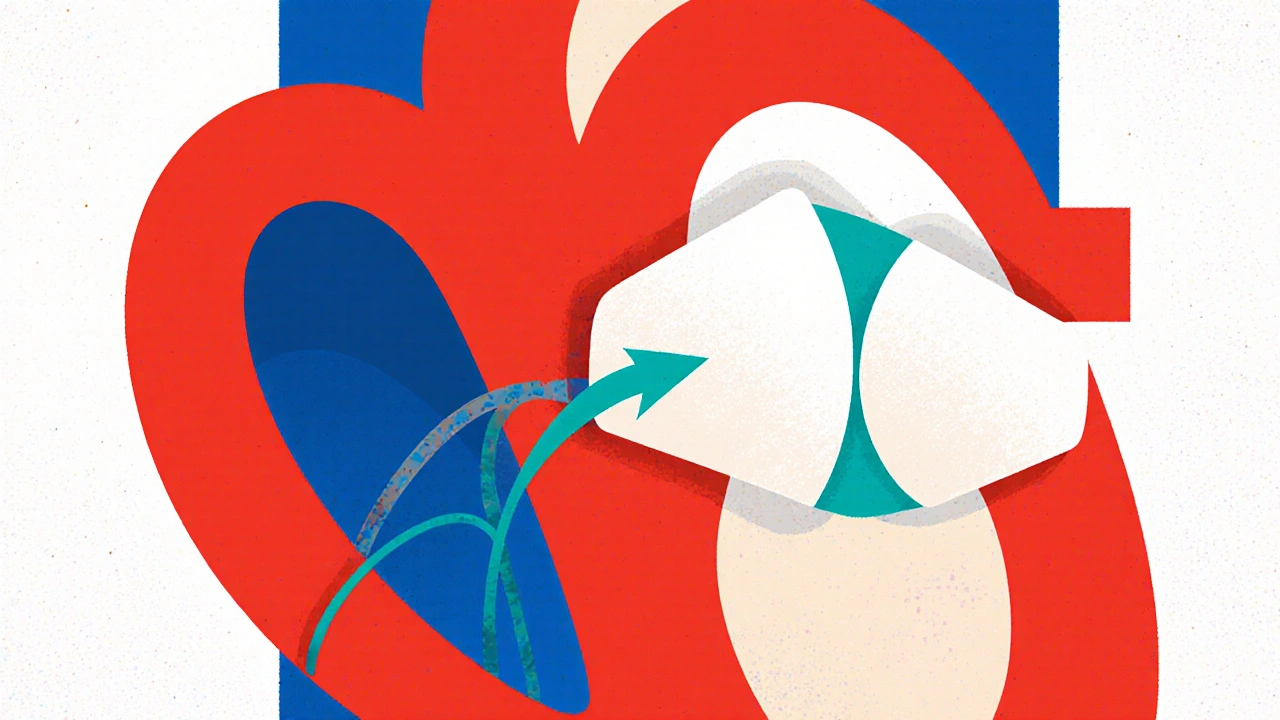
Heart Anatomy That Links the Two Conditions
The Left Ventricle is the thick‑walled chamber responsible for pumping oxygenated blood into the systemic circulation works in tandem with the Mitral Valve a two‑leaflet structure that ensures one‑way flow from the left atrium to the left ventricle. The valve’s support system includes the annulus, chordae tendineae, papillary muscles, and surrounding myocardium. When the ventricle dilates or its walls become stiff, this entire apparatus is pulled out of alignment, allowing the leaflets to fail to coapt properly.
How Left Ventricular Dysfunction Triggers Mitral Regurgitation
There are three main pathways linking LVD to MR:
- Systolic dilation: In heart failure with reduced ejection fraction (HFrEF), the ventricle enlarges. The mitral annulus stretches, and the papillary muscles are displaced outward, creating a gap between the leaflets.
- Ischemic remodeling: After a coronary artery disease event, scar tissue can tether the papillary muscles unevenly, leading to asymmetric leaflet tethering.
- Diastolic stiffening: In heart failure with preserved ejection fraction (HFpEF), high left‑atrial pressures force the mitral leaflets apart during systole, even if the ventricle size is normal.
Regardless of the pathway, the result is “functional” mitral regurgitation-meaning the valve itself is structurally normal, but the surrounding heart geometry is compromised.
Clinical Picture: What Patients Typically Feel
Early LVD may be silent, but as MR develops, patients notice:
- Shortness of breath on exertion (due to pulmonary congestion from backward flow).
- Fatigue and reduced exercise tolerance (low cardiac output).
- Occasional palpitations or irregular heartbeat (atrial enlargement can trigger atrial fibrillation).
Physical exam often reveals a holosystolic murmur best heard at the apex, radiating to the axilla. The intensity can fluctuate with changes in afterload or preload, reflecting MR’s dynamic nature.
Diagnostic Workup - Seeing the Problem in Real Time
The cornerstone of evaluation is Echocardiography ultrasound imaging that visualizes heart chambers, wall motion, valve motion, and blood flow. Modern machines provide:
- 2‑D and 3‑D imaging for annular dimensions.
- Color Doppler to grade regurgitant jet area.
- Quantitative measures: effective regurgitant orifice area (EROA) and regurgitant volume.
- Strain imaging to detect subtle LV contractile deficits before overt dilation.
When echo windows are limited, a cardiac MRI can offer precise volumetrics and tissue characterization, especially to differentiate ischemic scar from viable myocardium.
Other tests include:
- BNP or NT‑proBNP levels - biomarkers that rise with increased wall stress.
- Coronary angiography if ischemic disease is suspected.
- Exercise stress echo to see how MR severity changes with exertion.
Management - From Meds to the Operating Table
Therapy follows a stepwise approach:
Medical Optimization
Guideline‑directed heart‑failure drugs can remodel the ventricle and often shrink the MR jet:
- ACE Inhibitors medications that block angiotensin‑converting enzyme, lowering afterload and promoting reverse remodeling.
- Beta‑blockers - reduce heart rate, improve filling time, and lessen sympathetic drive.
- Mineralocorticoid receptor antagonists - further reduce fibrosis.
- ARNI (sacubitril/valsartan) - newer agents with proven benefits in HFrEF.
For patients with HFpEF, aggressive blood‑pressure control and treatment of atrial fibrillation are key.
Device‑Based Therapies
When LVD persists despite meds, cardiac resynchronization therapy (CRT) can improve synchrony, lower LV volumes, and consequently decrease MR severity. Implantable defibrillators are added for patients at risk of sudden cardiac death.
Interventional & Surgical Options
If MR remains moderate‑to‑severe (EROA > 0.30 cm²) after optimal therapy, valve repair or replacement is recommended.
| Approach | Typical Candidates | Pros | Cons |
|---|---|---|---|
| Open Mitral Valve Repair | Patients with durable valve tissue, low surgical risk | Durable, restores native anatomy | Invasive, longer recovery |
| MitraClip (edge‑to‑edge) | High‑risk surgical patients, functional MR | Minimally invasive, rapid discharge | May leave residual MR, limited durability |
| Transcatheter Mitral Valve Replacement | Failed repair or severe annular calcification | Complete elimination of MR | Device size, risk of LVOT obstruction |
Choosing between repair and replacement hinges on valve anatomy, annular size, and the patient’s overall health. A heart team-cardiologist, cardiac surgeon, imaging specialist-makes the final call.
Prognosis and Follow‑Up
Patients whose MR improves after ventricular remodeling have better survival and quality of life. Persistent severe MR predicts higher hospital readmission rates and worse outcomes. Regular follow‑up with echo every 6‑12 months is standard, with earlier imaging if symptoms worsen.
Emerging therapies, such as ventricular assist devices (VADs) as a bridge to transplant, also affect long‑term outlook for those with end‑stage LVD and refractory MR.
Frequently Asked Questions
Can mitral regurgitation develop without left ventricular dysfunction?
Yes. Primary (or organic) MR occurs when the valve leaflets, chordae, or annulus are damaged by infection, rheumatic disease, or calcification, independent of LV function.
Is functional MR always reversible?
Not always. Early aggressive medical therapy can reverse mild-moderate MR, but severe annular dilation often requires a procedural fix.
How does pulmonary hypertension fit into the picture?
Elevated left‑atrial pressure from MR backs up into the pulmonary veins, raising pulmonary artery pressures. Chronic pulmonary hypertension can further strain the right ventricle, creating a vicious cycle.
When is a MitraClip preferred over surgery?
In high‑risk surgical candidates-elderly patients, those with significant comorbidities-or when the MR is purely functional, a MitraClip offers a safer, quicker alternative.
What lifestyle changes help both conditions?
Low‑sodium diet, regular aerobic activity (as tolerated), weight control, and strict management of hypertension and diabetes all reduce ventricular stress and slow MR progression.
Understanding the tight link between left ventricular dysfunction and mitral regurgitation empowers patients and clinicians to intervene early, choose the right treatment path, and improve long‑term heart health.
sravya rudraraju
October 19, 2025 AT 19:17Left ventricular dysfunction fundamentally alters the geometric relationship between the papillary muscles and the mitral leaflets, thereby predisposing the valve to functional regurgitation.
When systolic failure induces ventricular dilatation, the mitral annulus expands outward, creating a spatial gap that prevents adequate coaptation of the leaflets.
Simultaneously, the displacement of the papillary muscles exerts tethering forces on the chordae tendineae, further limiting leaflet closure.
In diastolic heart failure, elevated left‑atrial pressures augment the trans‑mitral pressure gradient during systole, which can push the leaflets apart even in the absence of overt dilation.
Modern three‑dimensional echocardiography permits precise quantification of annular dimensions and leaflet stress, facilitating early identification of the functional mechanisms at play.
Strain imaging adds incremental value by detecting subtle reductions in myocardial contractility before gross volumetric changes become evident on two‑dimensional studies.
From a therapeutic standpoint, guideline‑directed medical therapy remains the cornerstone, as agents such as ACE inhibitors and mineralocorticoid receptor antagonists promote reverse remodeling of the ventricle.
Successful remodeling frequently translates into a measurable reduction in effective regurgitant orifice area, thereby delaying or obviating the need for interventional procedures.
In cases where optimal medical therapy fails to achieve sufficient reverse remodeling, cardiac resynchronization therapy can improve ventricular synchrony and modestly decrease regurgitant volume.
When the residual regurgitation remains moderate to severe, patient selection for percutaneous edge‑to‑edge repair versus surgical repair must consider annular size, leaflet integrity, and procedural risk.
The MitraClip device, while minimally invasive, may leave residual jet and requires careful post‑procedure surveillance with serial echocardiography.
Open surgical repair, conversely, offers the advantage of annuloplasty rings that restore annular geometry, but it carries higher peri‑operative morbidity, especially in frail patients.
Emerging transcatheter mitral valve replacement technologies aim to provide a definitive solution for patients unsuitable for repair, yet issues such as left ventricular outflow tract obstruction persist.
Regular follow‑up, ideally every six to twelve months, allows clinicians to monitor changes in ventricular volumes, regurgitant severity, and pulmonary pressures.
Ultimately, a multidisciplinary heart team approach that integrates imaging expertise, interventional skill, and heart‑failure management is essential for optimizing outcomes in patients with concomitant left ventricular dysfunction and functional mitral regurgitation.
Ben Bathgate
November 7, 2025 AT 00:17So you're telling me that meds alone fix the leak? In reality, I see a lot of patients who still end up needing a clip after years on ACE inhibitors. The guidelines are optimistic, but real‑world data shows high re‑operation rates. Bottom line, don’t ignore the anatomy.
Ankitpgujjar Poswal
November 25, 2025 AT 06:17Listen, if you’re still pushing beta‑blockers without checking remodeling, you’re missing the point. Get a 3‑D echo, assess annular size, and consider CRT now before the valve gets worse. Time is ventricle!
Rakhi Kasana
December 13, 2025 AT 12:17The heartbreak of watching a patient gasp for air while their own heart betrays them is beyond words. Functional MR may seem harmless on an echo, but it steals quality of life. We must intervene before despair sets in.
Catherine Viola
December 31, 2025 AT 18:17One must scrutinize whether the prevailing consensus on early MitraClip deployment adequately accounts for long‑term structural integrity. Evidence suggests that annular dynamics may render percutaneous solutions suboptimal in certain phenotypes.
Nicole Boyle
January 19, 2026 AT 00:17LV remodeling index correlates inversely with EROA progression.
Caroline Keller
February 6, 2026 AT 06:17Honestly this whole thing is just heart drama enough to make anyone cry. It’s a tragedy that so many ignore simple lifestyle fixes. Low‑salt diets and walking should be prescription, not optional. Wake up before the valve collapses.
dennis turcios
February 24, 2026 AT 12:17While the mechanistic link is clear, the decision matrix for intervention remains nuanced. A patient‑centered approach weighing comorbidities is indispensable.